Graft
Immediate Implant Placemen
IMMEDIATE IMPLANT PLACEMENT
Sulcular and submarginal incision, involving 2 teeth distal to the tooth to be extracted. No vertical incisions are performed.
Soft tissue margin of the tooth to be extracted more apically placed than the homologous natural tooth
IMPLANT POSITION
VERTICAL: 3 to 4mm from the soft tissue margin (dictated by adjacent teeth)
BUCCO-LINGUAL: outer surface of the implant 2mm to 3mm palatally to the bone envelope
Suture the graft to the inner surface of the flap, as if it was a marionette suture.
PROCEDURE
Incision the papillae: split thickness leaving a good amount of connective tissue on the anatomical papillae
After that dissect along the buccal bone full thickness
After the flap is detached from the buccal bone we go again split thickness beyond the mucogingival junction, first periosteal releasing incision is a conventional deep one, then, with the blade parallel to the mucosa and keeping it very superficial, detaching the muscles that are attached to the alveolar mucosa, you can see the blade through the transparency of the mucosa.
ANATOMICAL PAPILLAE DESEPITHELIALIZATION
First with the blade and then microsurgical scissors
Zuchelli arta tarde 1, very important from minute 1’20’’
SOFT TISSUE GRAFT
Should be placed, ideally, 1mm more coronal than the soft tissue margin, sutured to the base of the anatomical papillae - this isn’t a problem on the delayed approach.
Should include both mesial and distal papillae
The flap should completely cover the graft
Suture the graft to the inner surface of the flap on the immediate implant placement
Anatomical papillae are more fragile, because they belong to the extracted tooth, so on immediate implant placement we are not suturing the graft to the anatomical papillae, we are suturing the graft to the base of the surgical papillae:
Base of the surgical papilla (entry at the buccal) - graft - needle back through the inner surface of the flap - knot
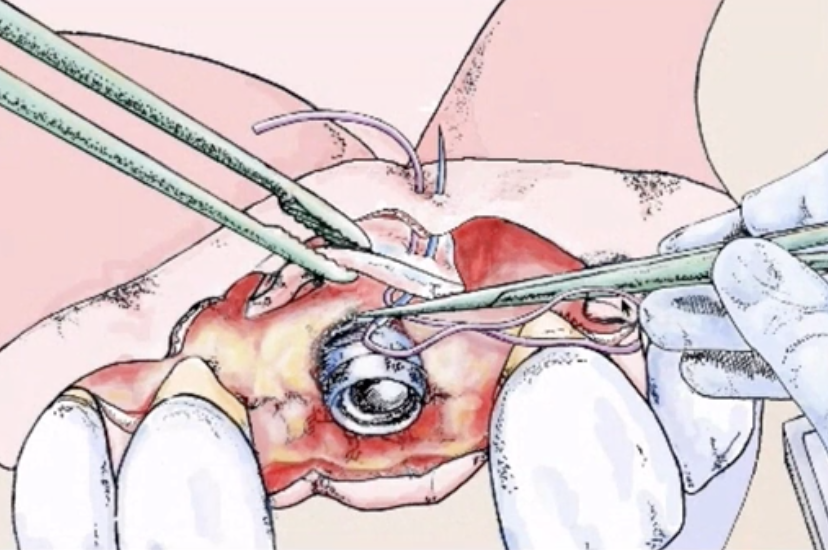
Horizontal mattress suture
This allows a submarginal positioning of the graft and the inner aspect of the surgical papillae will be entirely available to join the outer aspect of the anatomical desepithelialized papillae.
Only the flap will advance maintaining the graft 1mm apical to the soft tissue margin, this will promote papilla growth in thickness at first and then in height (creeping).
Sling suture around adjacent teeth to CAF
Very important from minute 2’05’’
Perforate buccal mesial - sling - perforate buccal distal - sling - knot
Suture of the papillae of the implant site is last:
2 single sutures one shot perforates buccal and palatal, one at the mesial papilla and the other at the distal papilla.
The second suture to make the flap advancement sling suture